Radiography has a modest place in the diagnosis and management of patients with cirrhosis, being used, for example, in screening for ascites, shown below, seeking evidence of bowel perforation in patients with suspected bacterial peritonitis, and monitoring bowel distension in acutely ill patients admitted for treatment of decompensation or variceal hemorrhage.
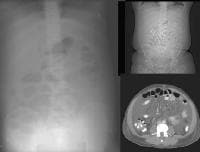 A 51-year-old male who has cirrhosis with massive ascites. On kidney, ureters, bladder (KUB), and digital scout view, small bowel loops are seen primarily in the midabdomen. The abdomen appears hazy. A computed tomography (CT)–scan axial view confirms the presence of small bowel loops floating centrally in ascitic fluid and of the existence of fluid in paracolic gutters.
A 51-year-old male who has cirrhosis with massive ascites. On kidney, ureters, bladder (KUB), and digital scout view, small bowel loops are seen primarily in the midabdomen. The abdomen appears hazy. A computed tomography (CT)–scan axial view confirms the presence of small bowel loops floating centrally in ascitic fluid and of the existence of fluid in paracolic gutters.Routine chest radiography in a patient with cirrhosis may demonstrate elevation of the diaphragms from ascites. Gynecomastia may be appreciated. The azygos vein may be enlarged because of collateral flow, as in the first image below, and pleural effusions, shown below, may occur from the presence of pleuroperitoneal fistulas.
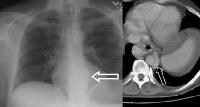
 Shunts may occur by way of the retroperitoneum and azygos pathways. A chest radiograph on a patient with such a configuration demonstrates an enlarged azygos vein at the level of the azygos arch (arrow). This can also be appreciated on a localizer magnetic resonance imaging (MRI) scan in the sagittal plane.
Shunts may occur by way of the retroperitoneum and azygos pathways. A chest radiograph on a patient with such a configuration demonstrates an enlarged azygos vein at the level of the azygos arch (arrow). This can also be appreciated on a localizer magnetic resonance imaging (MRI) scan in the sagittal plane. A 48-year-old male with cirrhosis from hepatitis C with intractable ascites and pleural effusion. Chest radiograph obtained 1 day prior to a scintigraphic study shows right-sided pleural effusion.
A 48-year-old male with cirrhosis from hepatitis C with intractable ascites and pleural effusion. Chest radiograph obtained 1 day prior to a scintigraphic study shows right-sided pleural effusion.Rarely, giant esophageal varices may be appreciated as a soft-tissue mass at the gastroesophageal junction, as in the image below.
 An abnormal soft-tissue density is seen (arrow) in the lower mediastinum, superimposed over the shadow of the descending aorta. This density represents massively dilated esophageal varices on the corresponding computed tomography (CT) scan (arrow), just above the level of the left hemidiaphragm, immediately adjacent to the aorta.
An abnormal soft-tissue density is seen (arrow) in the lower mediastinum, superimposed over the shadow of the descending aorta. This density represents massively dilated esophageal varices on the corresponding computed tomography (CT) scan (arrow), just above the level of the left hemidiaphragm, immediately adjacent to the aorta.An upper GI study can demonstrate varices at the gastroesophageal junction, depicted below, but for the most part, endoscopy has superseded fluoroscopic techniques.
 Varices at the gastroesophageal junction (arrow), demonstrated on an upper GI series. The varices become more prominently seen on Valsalva maneuver. A computed tomography (CT) scan in the same patient shows enhancing collateral vessels.
Varices at the gastroesophageal junction (arrow), demonstrated on an upper GI series. The varices become more prominently seen on Valsalva maneuver. A computed tomography (CT) scan in the same patient shows enhancing collateral vessels.Plain film findings are generally confirmed by other imaging modalities or by clinical evidence.
Tidak ada komentar:
Posting Komentar